Hypertrophic cardiomyopathy (HCM), the most common of the genetic cardiovascular diseases, is characterized by heterogeneous clinical expression, unique pathophysiology and a diverse clinical course. Sudden cardiac death, progressive heart failure, atrial fibrillation and stroke are leading causes of the morbidity and mortality associated with HCM.
| Clinical Features | HCM manifests at any age, from young children to the elderly. Symptoms include dyspnea, angina pectoris, fatigue, syncope and palpitations. Clinical evaluation is usually triggered in response to symptoms suggestive of HCM, or in asymptomatic individuals to investigate a systolic murmur, ECG abnormalities, or during family screening.HCM is characterized by a thickened, but non-dilated left ventricle in the absence of another cardiac or systemic condition such as, aortic valve stenosis, systemic hypertension and some forms of athlete’s heart that is capable of producing the extent of hypertrophy. |
| Incidence | 1:200 |
| Genetics | Currently, 14 different genes encoding sarcomeric proteins are implicated in HCM. |
Genes Associated with HCM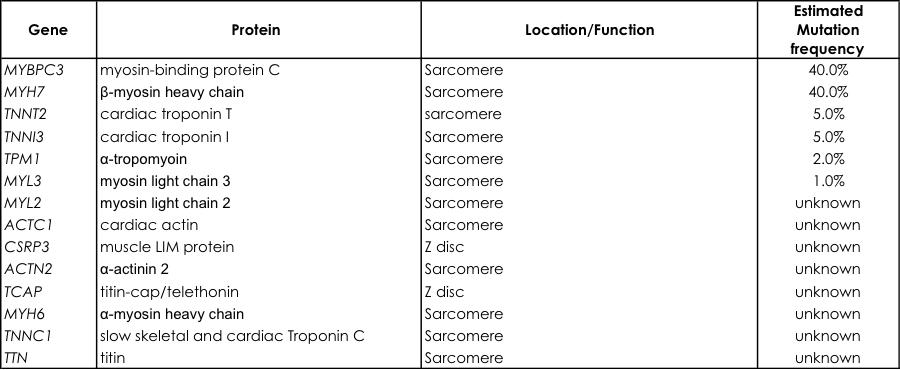 |
|
| Inheritance | Autosomal dominant |
| Penetrance | Incomplete with variable expression |
| Disease Pathogenesis | Pathogenic variants in nearly all sarcomere proteins lead to increased actin-activated ATPase activity, disruption of actin-myosin interaction and force generation, and altered intracellular calcium signaling in cardiomyocytes. |
| Clinical Utility | Early diagnosis Phenotype prediction Clinical management of at-risk realtives Risk stratification |
| Indications for Molecular Testing | Comprehensive or targeted (MYBPC3, MYH7, TNNI3, TNNT2, TPM1) HCM genetic testing is recommended for any patient in whom a cardiologist has established a clinical diagnosis of HCM based on examination of the patient’s clinical history, family history, and electrocardiographic/echocardiographic phenotype. Mutation-specific genetic testing is recommended for family members and appropriate relatives following the identification of the HCM-causative mutation in an index case.Disease processes other than HCM, like the cardiac predominant variant of Fabry disease (GLA-HCM), Danon disease (LAMP2-HCM) or Wolf-Parkinson-White syndrome (PRKAG2-HCM) can lead to the common finding of left ventricular hypertrophy. These diseases have different prognoses and clinical management strategies. |
| Test Information | MYBPC3, MYH7, TNNT2, TNNI3, TPM1, ACTC1, MYL2, MYL3, LAMP2, GLA, PRKAG2, TTR Gene exons and intron/exon boundaries are analyzed subsequent to Sanger sequencing. Mutations detected by sequence analysis may include small intragenic deletions/insertions and missense, nonsense, and splice site mutations. Exonic or whole-gene deletions/duplications will not be detected. Additionally, a negative result does not rule out causal gene mutations as the promoter region and cryptic splicing mutations are not investigated. |
| Clinical Sensitivity | 40% – 65% |
| Turnaround time | 6-8 weeks |
| CPT Codes | 81404 x 1, 81405 x 7, 81406 x 2, 81407 x 2 |
Sample and Shipping Information
| Specimen | Whole blood drawn in lavender top (EDTA) tube in a volume of 3-5cc (Adults/Children) and 3 cc (infant |
| Shipping | Refrigerate sample until time of shipping. Ship sample at room temperature in an insulated container by overnight delivery. |
| Causes for Rejection | Frozen specimen; hemolysis; quantity not sufficient for analysis; improper container. |
References
Teekakirikul P, Kelly MA, Rehm HL, Lakdawala NK, Funke BH. Inherited cardiomyopathies: molecular genetics and clinical genetic testing in the postgenomic era. J Mol Diagn. 2013 Mar;15(2):158-70.
Ackerman MJ, Priori SG, Willems S, Berul C, Brugada R, Calkins H, Camm AJ, Ellinor PT, Gollob M, Hamilton R, Hershberger RE, Judge DP, Le Marec H, McKenna WJ, Schulze-Bahr E, Semsarian C, Towbin JA, Watkins H, Wilde A, Wolpert C, Zipes DP; Heart Rhythm Society (HRS); European Heart Rhythm Association (EHRA). HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies: this document was developed as a partnership between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA). Europace. 2011 Aug;13(8):1077-109.
Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB; American Heart Association; Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; Council on Epidemiology and Prevention. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention.
Circulation. 2006 Apr 11;113(14):1807-16.
Resources
American Heart Association (AHA)
7272 Greenville Avenue
Dallas TX 75231
Phone: 800-242-8721 (toll-free)
review.personal.info@heart.org
www.americanheart.org
Children’s Cardiomyopathy Foundation (CCF)
PO Box 547
Tenafly NJ 07670
Phone: 866-808-2873 (toll-free)
Fax: 201-227-7016
info@childrenscardiomyopathy.org
www.childrenscardiomyopathy.org
Hypertrophic Cardiomyopathy Association (HCMA)
328 Green Pond Road
PO Box 306
Hibernia NJ 07842
Phone: 973-983-7429
Fax: 973-983-7870
support@4hcm.org
www.4hcm.org